
Page 247 - tmp
P. 247
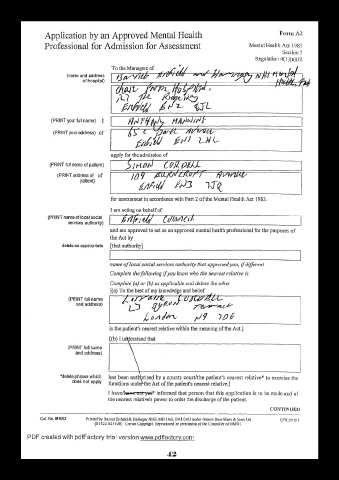
Application by an Approved Mental Health Form A2
Professional for Admission for Assessment Mental Health Act 1983
Section 2
Regulation 4(1 )(a)(ii)
(name and address
of hospital)
(PRINT your full name) I
(PRINT your address) of
(PRINT full name of patient)
(PRINT address of of
patient)
(PRINT name of local social
services authority)
and am approved to act as an approved mental health professional for the purposes of
the Act by
delete as appropriate [that authority]
(PRINT full name
and address)
[(b) I understand that
(PRINT full name
and address) \
CONTINUED
PDF created with pdfFactory trial version www.pdffactorv.com
42